
This month begins my series on J-Pouches. I have spent many months researching and many hours putting all these posts together to get a better understanding of J-Pouches so that I might share the information with you. I hope that you enjoy my five-part series on the J-Pouch. This week I share J-Pouch History.
J-Pouch History
1933
The first attempted ileoanal anastomosis was performed by Dr. Rudolph Nissen (also spelled Rudolf Nissen) of Berlin in 1933. Nissen performed the procedure on a 10-year-old with polyposis with reportedly great results. In 1948, doctors at Johns Hopkins Hospital, Mark Ravitch and David Sabiston, experimented with ileoanal anastomosis and anorectal mucosectomy on 28 dogs. Through their trial and error, they found that this technique was implemented with great results. Ravitch then used this technique on two ulcerative colitis (UC) patients who had very successful results.
1948-1955
Between 1948 and 1955, various doctors continued to experiment with this technique. They found that the biggest problem was frequent bowel movements, dehydration, electrolyte imbalance, fistulas and abscesses. M. A. Valiente and H. E. Bacon believed these complications could be remedied by creating a reservoir, stating, “It is our belief that if an adequate pouch can be obtained and the sphincter mechanism can be preserved intact, it would be possible for these patients to retain the ideal contents enough so that only three to four bowel movements take place every day.”
Through their experiments with seven dogs, two of them were successful. However, five other dogs died making these results somewhat disappointing.
1969
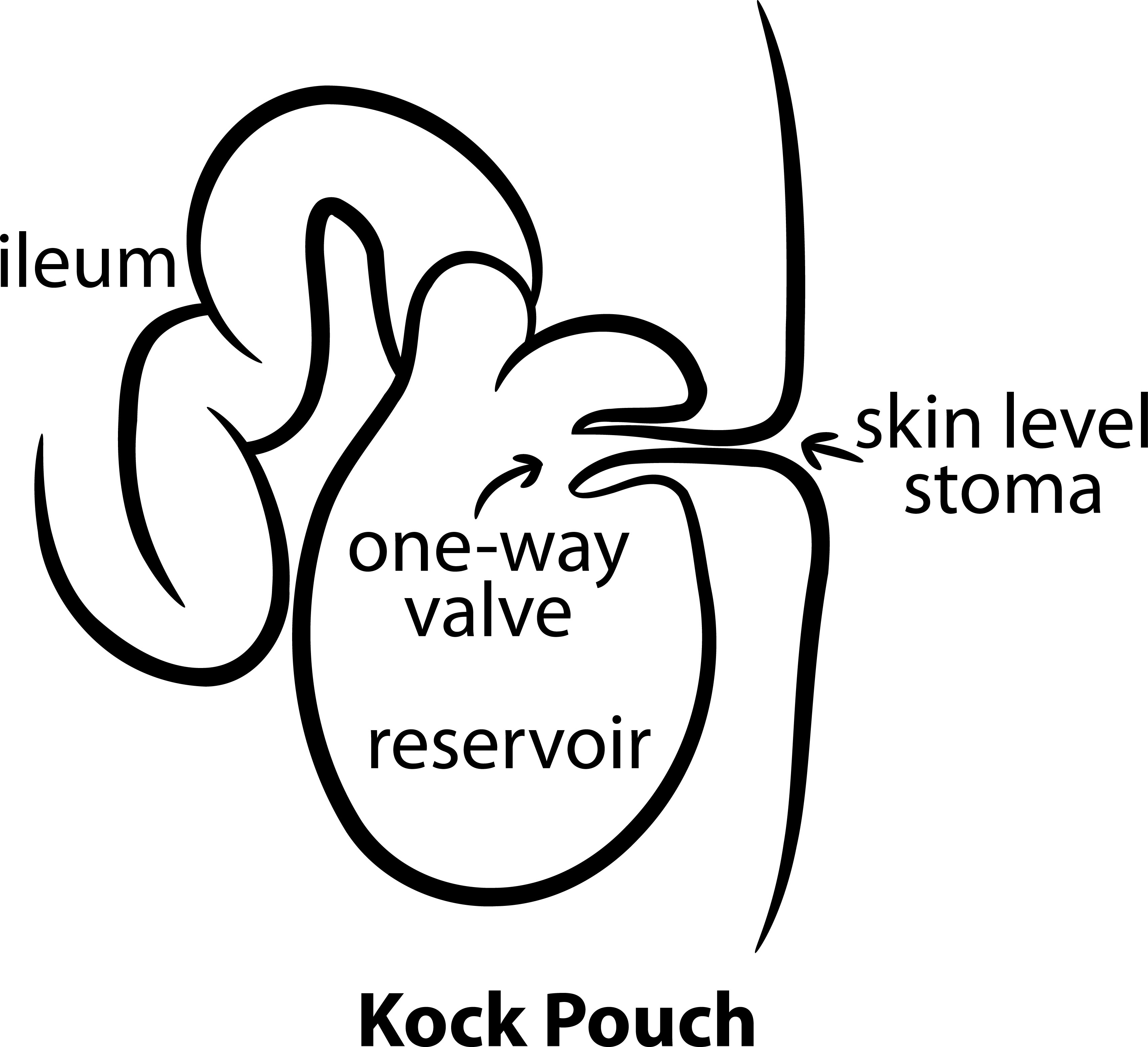
 In 1969, a Swedish surgeon by the name of Dr. Nils Kock made the first continent intestinal reservoir. This pouch was called the Kock Pouch and by the early 1970’s, this technique was widely used in the United States with UC and familial adenomatous polyposis (FAP). There were complications that came along with the Kock Pouch, however. Those included valve slippage and leaks.
In 1969, a Swedish surgeon by the name of Dr. Nils Kock made the first continent intestinal reservoir. This pouch was called the Kock Pouch and by the early 1970’s, this technique was widely used in the United States with UC and familial adenomatous polyposis (FAP). There were complications that came along with the Kock Pouch, however. Those included valve slippage and leaks.
1970s & 1980s
In the 1970s and 1980s, two groups that were working independently produced great results in ileal-pouch anal anastomosis technique. The first was a group supervised by Dr. A. G. Parks who was the chief surgeon at St. Mark’s Hospital and the London Hospital. He recorded 21 patients in 1980 who were treated with the ileal-reservoir anal anastomosis for both UC and FAP.
Dr. Parks’ version of the ileal-reservoir consisted of the S-Pouch with a temporary loop ileostomy. As with many procedures, greater experience yields greater results. His first patients had a 70% complication rate that soon decreased to about 20%. Eighteen out of 20 patients had no trouble with mucus leakage and all of the patients were continent.

(Click to see larger version.)
Around the same time, a Japanese doctor at the Tokyo Medical and Dental University named J. Utsunomiya was experimenting with the J-Pouch. His team described 3 different types of anastomosis with each of the three having a temporary loop ileostomy. Of the three different types, the most successful was the antiperistalic J-Pouch patients. However, all of his patients showed great progress and complete stool continence.
The 1980s showed great promise for the ileal-pouch anal anastomosis. With a better understanding of the rectal anatomy and improvement in surgical staplers, great progress was made for the treatment of UC.
1995
Dr. Victor Fazio at Cleveland Clinic Foundation and his team have played some very key roles in the 1995 detailed study of patient outcomes in double-stapled J-Pouch surgery. In the study, Fazio and his team found that early complications were commonly small bowel obstructions, wound infections, pouch abscesses, and pouch bleeding. Late complications such as pouchitis, small bowel obstruction and anal stricture occurred most commonly. This study, which involved 1,005 patients, showed that 93% reported a better quality of life. Therefore, the operation was considered successful and safe for most patients.
Today, the success rates are higher than ever and J-Pouch failure continues to drop. As with anything, the more experience the greater the results. While surgery is far from being the most ideal treatment for ulcerative colitis, I feel like the future is very bright in the treatment for UC.
***


SOURCES:
Parks, A. G., and R. J. Nicholls. “Proctocolectomy without Ileostomy for Ulcerative Colitis.” Bmj 2.6130 (1978): 85-88. Web.
Dozois, R.r. “Ileal ‘J’ Pouch–anal Anastomosis.” Frontiers in Colorectal Disease (1986): n. pag. Web.
Melville, D. M., J. K. Ritchie, R. J. Nicholls, and P. R. Hawley. “Surgery for Ulcerative Colitis in the Era of the Pouch: The St Mark’s Hospital Experience.” Gut 35.8 (1994): 1076-080. Web.
Onaitis, Mark W., and Christopher Mantyh. “Ileal Pouch-Anal Anastomosis for Ulcerative Colitis and Familial Adenomatous Polyposis.” Annals of Surgery 238.Supplement (2003): n. pag. Web.
Mcguire, B. B., A. E. Brannigan, and P. R. O’connell. “Ileal Pouch–anal Anastomosis.” British Journal of Surgery Br J Surg 94.7 (2007): 812-23. Web.
Scoglio, Daniele. “Surgical Treatment of Ulcerative Colitis: Ileorectal vs Ileal Pouch-anal Anastomosis.” World Journal of Gastroenterology WJG 20.37 (2014): 13211. Web.

I had UC and 3 major surgeries with colectomy. I have J-Pouch. It is a great procedure in surgical. Thank you, Dr. Elizabeth Breen, at BWH in Boston, MA. She is a great surgeon! God Bless!!
I have an ileostomy and have been told the j-pouch is not a good option for me. They said since my stool is so liquid I would have a lot of leakage and would get extremely sore.
Hi Karen! I’m sorry to hear that. Sending hugs your way. <3
I’ve had my J pouch for 6 years now. It’s been a life saver!! I love it and I’m so grateful for the procedure! ❤️
Same here, Mari! I’m so grateful for mine. I’ve only had it for 2 years.
Thank you for this, very informative. I’m on my 2nd J-pouch, got my first (defective) one in 1995. (I didn’t realize it was right after they had just pretty much figured out the gritty details). I just got my second one this past March and unfortunately I’m experiencing a lot of mucosal leaking ~ didn’t have any the first time, so I’m kind of scared this one isn’t going to work. But I’m keeping my fingers crossed 😉.
Good luck! Keeping you in my thoughts and prayers!
Yes, I agree (awesome info). It is great to see the success rate so high as I hope mine will go well. I have had complications in the second round as they built the pouch April 6th. Take down is 11 days away. Thanks for your efforts and work.
Good luck! Let me know how it works out for you if you think about it! 🙂
Thanks for posting. I have had my j-pouch since 2000, and love the great quality of life I have thanks to it!
That’s great! Thanks! I’ve had mine for two years now, and so far I’m happy with it.
Well done, intestine reading 😉 sorry interesting 😂
This is excellent information. I have had my jpouch for 3 years. It saved my life to be somewhat normal. You have done a great job putting this blog together. I look forward to reading the future ones.
Thank you, Hope! I appreciate you reading it! I’ve had my j-pouch for 2 years so I’m not far behind you at all! 🙂